Urinary tract infections (UTIs) are a very common issue, seen in all areas of healthcare. It is about 4 times more common in women than in men, usually between the ages of 20-24. However, there is also a spike noted in men over the age of 84.

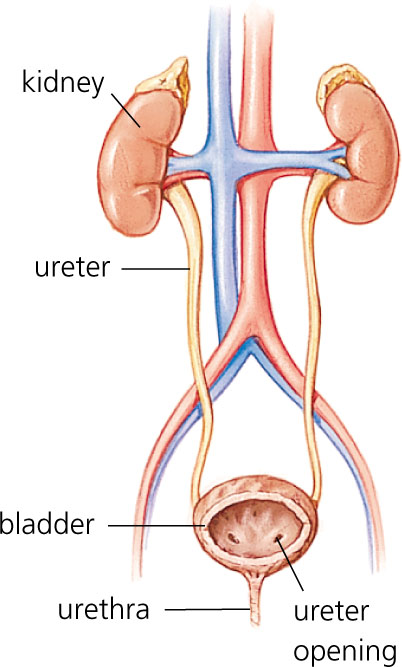
The urinary tract is made up of (moving from the entry up) urethra, bladder, ureters and kidney. Each site has it’s own name for when it is affected, i.e. urethritis, cystitis, ureter infection and pyelonephritis, respectively. The information below should not bypass any diagnosis given by your physician as individuals feel pain and discomfort in different
The reason urinary tract infection are more commonly seen in women is that the typical female urethra is approximately 4 cm in length while the male urethra’s length will vary from 15-29 cm (depending on the study). Nevertheless, the women’s urethra is substantially shorter allowing it to be at higher risk for ascending infections.
Typical symptoms include pain or burning sensation when urinating (called dysuria), a sense of needing to frequently urinate (frequency), passing small amounts of urine when the urge to urinate is high (urgency) and lower abdominal pain can be present. Cloudy urine can either be a sign of purulent material (bacteria) in the urine or a sign that someone is dehydrated. Commonly during urinary tract infections, blood is present in the urine. This may be visible in the urine (called hematuria) or it may be invisible to the naked eye, requiring use of a urine dipstick (normally present in most physician offices).
It should be noted that these typical symptoms may not be the ones present for all patients but a patient self diagnosis was noted to have a positive predicted value of 85.7% in a high quality study by Bent and al. noted in JAMA 2002, 287:2701. What this means is that when patients said, “Hey Doc! I think I have a urinary tract infection, 85.7% of the time, they were right.” In comparison, having blood in the urine gave a positive predictive value (PPV) of 75%, and having pain when urinating gave a PPV of 69.2%! “When you know, you just know.”
Now having said that, the more serious pyelonephritis (kidney infection) may show up differently with symptoms of fever, chills, nausea and vomiting and complaints of pain in the back along the side (“flank pain”). On exam, health care providers can assess costovertebral angle tenderness. These signs and symptoms, with or without signs/symptoms of urinary tract infection increase the likelihood that there is a pyelonephritis.
When men (especially elderly men) present with infection, they will present with symptoms of foul smelling odour, nausea and gross hematuria (meaning you can see the blood not the other kind of gross…. though both work.)
As alluded to previously, some of the more common tests that can be done include the “urine dipstick”, which can give a quick hit answer in the office. It has essentially replaced the use of in office microscopy and there is no need to have patients do a “clean catch urine”, which is where the patient will start urinating then start catching the urine mid stream. Messy work, and so most patients are happy to be done with it, and also it commonly was not done completely accurately, making them more of a false sense of security that the specimen collected is a proper specimen.
Having either a positive “Leukocyte Esterase” or “Nitrite” or both can be enough for a diagnosis and usually is enough to initiate treatment. Based on the work by Deville and al. in BMC Urology 2004, 4(1): 4, it was noted that there is a high chance that a child, pregnant woman or elderly patient does not have a urinary tract infection if both the nitrite and leukocyte esterase is normal. In everyone else, having these tests showing as negative, does not rule out a UTI. Usually, the confirmatory test is a urine culture.
The urine culture is quite an interesting test, as it can provide with great information as it not only states what the bacteria is, but also with the names of the medications with which it is sensitive.
Seventy to ninety percent of the time, the causative bacteria is E. Coli, while the others involved include Staphylococcus saprophyticus, proteus, klebsiella and enterococcus. Sometimes there are also mixed samples noted as well, which typically mean that the sample has been contaminated, usually by a non-sterile container. This is usually the case when people bring in samples from home, understandable as they would like to limit the amount of time they will be urinating until treated.
There is a phenomenon called asymptotic bacteriuria, in which bacteria is noted in the urine on “screening” tests or because the urine was checked for another reason and there is no symptoms associated with it. This practice should not be done unless it is on a pregnant patient where the bacteria can cause problems with the pregnancy. The only other exception is if there is subtyping done on the bacteria, which notes that the E. Coli has O or K subtype, which is notorious for causing pyelonephritis.
Treatment is with a myriad of antibiotics and the choice is usually more dependant on provider choice and patient allergies. The biggest qualm I have is with providers that still give long courses for women with uncomplicated cystitis. Antibiotics should be given for 3-5 days (unless it is nitrofurantoin which should be given for 7 days). This is based on high quality studies and SORT A.
Exceptions to above will be in men and in pyelonephritis, the course should be for 7-14 days for men with UTIs and 10-14 days (SORT C) for pyelonephritis. If the pyelonephritis is severe, it may require hospitalization and possibly intravenous antibiotics. It should be noted that patients that can tolerate medications by mouth, should use as such, as there are no less effective than taking the medication through an intravenous route.
So what about just preventing them all together? Eat a lot of cranberries, right? At this time, cranberry juice has not been shown to be effective in treating UTIs, however there is some evidence that women that drink cranberry juice may have less symptomatic urinary tract infections. It should be noted that the same studies have high numbers of dropouts which might mean that using cranberry juice long term may not be a feasible choice. As always in medicine, more studies are required.